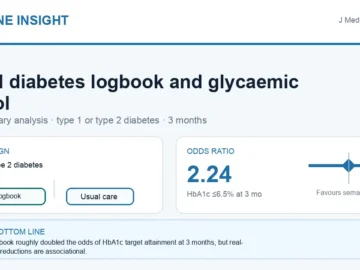
Can a Digital Logbook Improve Blood Sugar Control in Diabetes?
A manufacturer-sponsored secondary analysis found a digital diabetes logbook nearly doubled the odds of reaching HbA1c 6.5% or below at 3 months, with associated real-world glucose reductions. PICO summary and expert commentary.