

Summary: In adults with chronic kidney disease, type 2 diabetes, and albuminuria receiving renin-angiotensin system blockade, simultaneous finerenone plus empagliflozin reduced UACR more than finerenone or empagliflozin alone at 180 days. The trial assessed a surrogate kidney marker rather than clinical kidney failure or cardiovascular events.
PICO Summary
| Element | Detail |
|---|---|
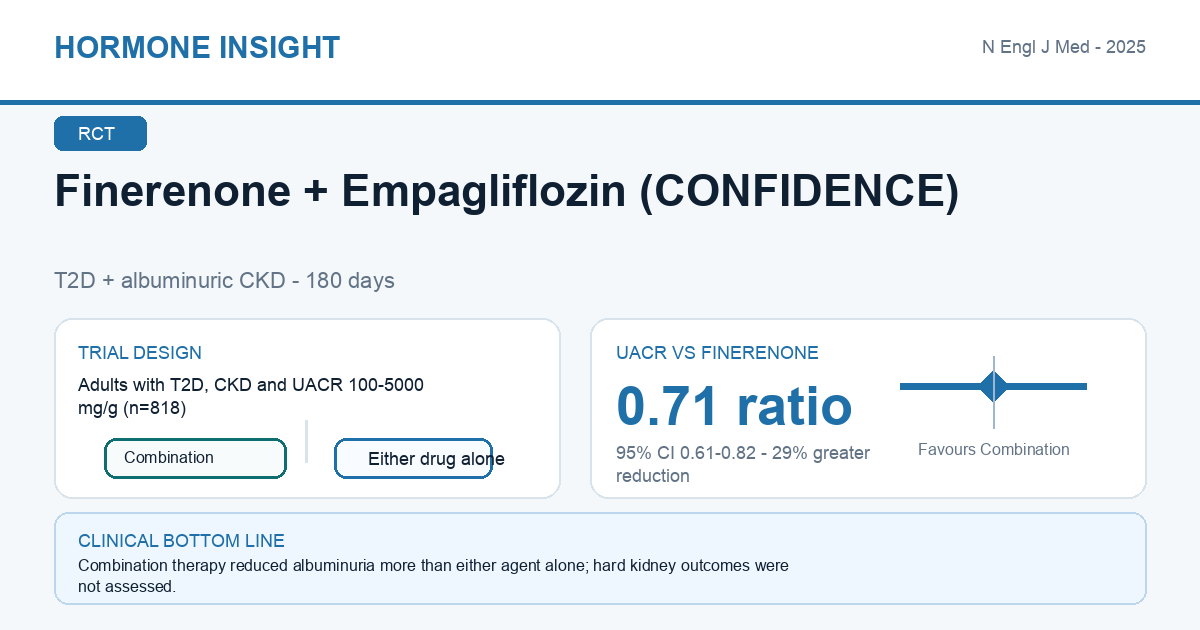
| Population | 818 adults with type 2 diabetes, CKD (eGFR 30-90 mL/min/1.73 m2), and UACR 100-5000 mg/g receiving a renin-angiotensin system inhibitor; phase 2, double-blind, three-arm RCT. |
| Intervention | Finerenone 10 or 20 mg daily plus empagliflozin 10 mg daily (n=265 with baseline data). |
| Comparison | Finerenone alone (n=258) or empagliflozin alone (n=261), with matching placebo. |
| Outcome | At day 180, UACR reduction with combination therapy was 29% greater than finerenone alone (ratio 0.71, 95% CI 0.61-0.82) and 32% greater than empagliflozin alone (ratio 0.68, 95% CI 0.59-0.79); P<0.001 for both comparisons. |
Finerenone + Empagliflozin (CONFIDENCE)
Phase 2 RCT - T2D + albuminuric CKD - 180 days
Finerenone plus empagliflozin reduced UACR more than either agent alone at 180 days, with no unexpected safety signal; clinical kidney and cardiovascular outcomes were not tested.
Expert Commentary
CONFIDENCE provides the strongest randomized evidence so far for starting finerenone and an SGLT2 inhibitor together in albuminuric chronic kidney disease with type 2 diabetes. The additional UACR reduction was sizeable compared with either component alone, and the absence of an obvious excess of treatment-limiting hyperkalemia, acute kidney injury, or symptomatic hypotension is reassuring. The clinical interpretation still needs discipline: UACR is a validated risk marker, but this 180-day phase 2 trial was not designed to show fewer kidney-failure or cardiovascular events. Its participants also had substantial albuminuria despite renin-angiotensin system blockade, so extrapolation to lower-risk CKD is uncertain. Can I use this with my patients? Yes, for an appropriate patient with type 2 diabetes, persistent albuminuric CKD, adequate eGFR, and an indication for both drug classes, simultaneous or closely sequenced initiation is now evidence-supported if potassium, renal function, volume status, and blood pressure can be monitored. It should not be interpreted as permission to bypass contraindications or laboratory follow-up. The result strengthens a layered cardiorenal approach, but hard-outcome trials and longer safety follow-up remain important. In practice, the main change is greater confidence in combination initiation, not a new claim that albuminuria reduction alone guarantees improved survival or freedom from kidney failure.
References
Agarwal R, Green JB, Heerspink HJL, et al. Finerenone with Empagliflozin in Chronic Kidney Disease and Type 2 Diabetes. N Engl J Med. 2025;393(6):533-543. doi:10.1056/NEJMoa2410659. PMID: 40470996.