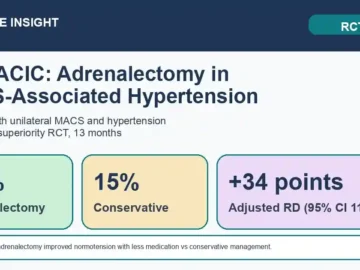
CHIRACIC Trial: Adrenalectomy Reduced Treatment Burden in MACS-Associated Hypertension
In CHIRACIC, adrenalectomy improved home-blood-pressure normotension with less medication versus conservative management in unilateral mild autonomous cortisol secretion-associated hypertension.